Sensibilidad al gluten/trigo: el camino hacia el diagnóstico
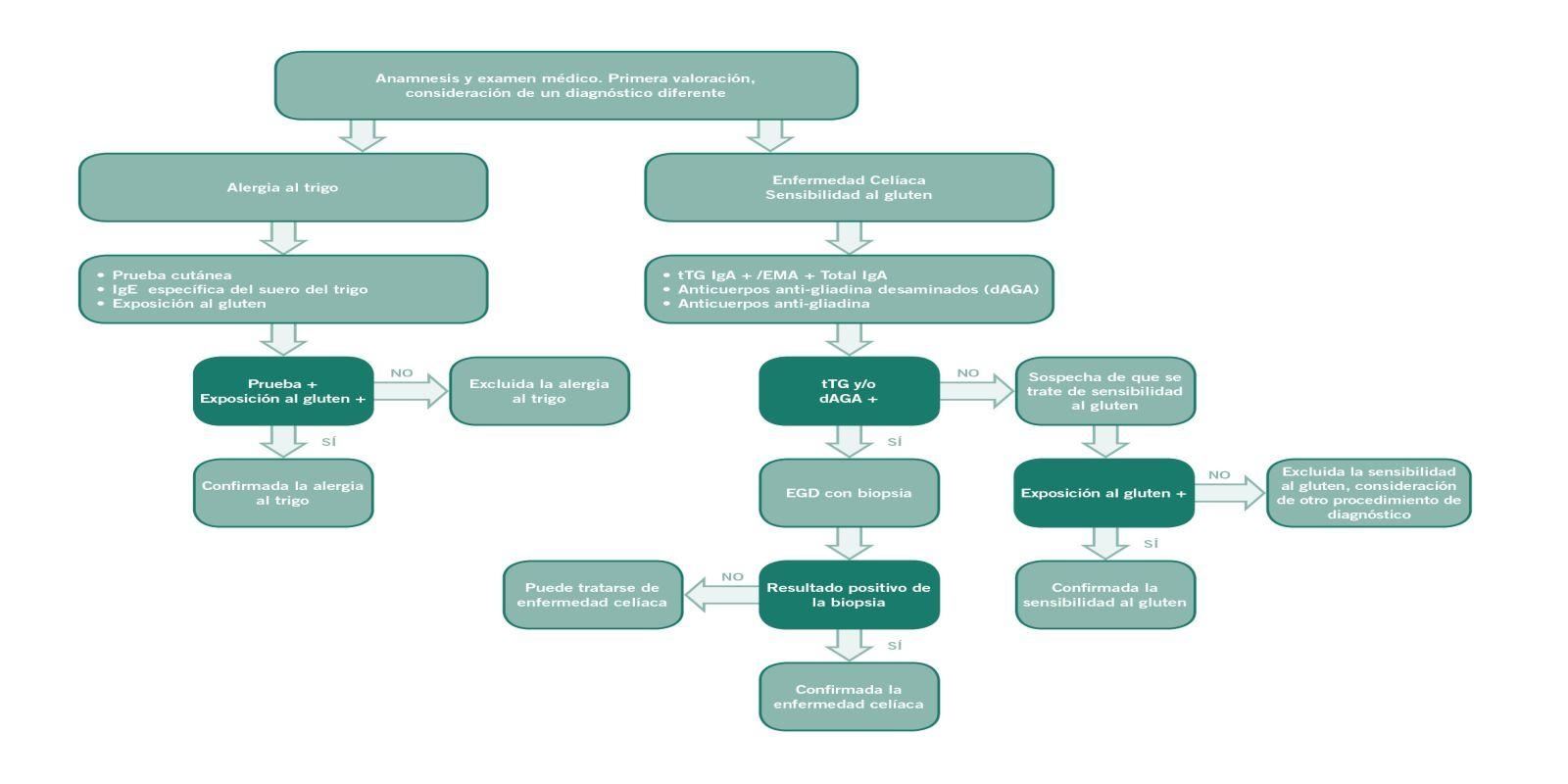
Para el diagnóstico de la sensibilidad al gluten/trigo, después de haber descartado la enfermedad celíaca y la alergia al trigo, se examina si una alimentación sin gluten proporciona mejoría.
Si tras el consumo de alimentos con gluten un paciente se queja de molestias no específicas, como dolor abdominal, dolor de cabeza o cansancio, en primer lugar hay que descartar la enfermedad celíaca y la alergia al trigo. Si estas dos enfermedades se descartan, hay que pensar en la sensibilidad al gluten/trigo. El diagnóstico se confirma a través de una mejoría o la desaparición de los síntomas al llevar una alimentación sin gluten y la recaída en cuando se vuelve a consumir gluten. Normalmente los síntomas mejoran en un plazo que va desde unos días a dos semanas. Es importante que el paciente no comience la dieta sin gluten hasta que un profesional de la salud se lo indique.
Anamnesis
Localizar los síntomas e indicios
En primer lugar es importante detectar si los síntomas que describe el paciente son típicos de la SG/T y si estos podrían estar relacionados con el consumo de alimentos con gluten. Antes de iniciar el proceso de diagnóstico, el paciente debería alimentarse por lo menos durante seis semanas de forma normal, es decir, sin excluir los alimentos con gluten.
En primer lugar es importante detectar si los síntomas que describe el paciente son típicos de la SG/T y si estos podrían estar relacionados con el consumo de alimentos con gluten. Antes de iniciar el proceso de diagnóstico, el paciente debería alimentarse por lo menos durante seis semanas de forma normal, es decir, sin excluir los alimentos con gluten.
Descartar la enfermedad celíaca
Prueba de anticuerpos específicos de la enfermedad celíaca y biopsia
Dado que las molestias de la SG/T se parecen a los de la enfermedad celíaca, es importante descartar esta última como primer paso para un diagnóstico correcto. Para ello, en primer lugar se lleva a cabo una prueba de anticuerpos, con la que también se debería descartar una carencia de IgA. Con la biopsia del intestino delgado adicional puede descartarse la enfermedad celíaca de forma definitiva. En la SG/T no se presenta una atrofia vellositaria, pero es probable que los valores de los LIE estén ligeramente elevados (Marsh 0-1).
Dado que las molestias de la SG/T se parecen a los de la enfermedad celíaca, es importante descartar esta última como primer paso para un diagnóstico correcto. Para ello, en primer lugar se lleva a cabo una prueba de anticuerpos, con la que también se debería descartar una carencia de IgA. Con la biopsia del intestino delgado adicional puede descartarse la enfermedad celíaca de forma definitiva. En la SG/T no se presenta una atrofia vellositaria, pero es probable que los valores de los LIE estén ligeramente elevados (Marsh 0-1).
Descartar la alergia al trigo
Prueba de anticuerpos de la IgE y prueba cutánea de punción
La alergia al trigo también puede parecerse a la SG/T por su cuadro clínico. Por eso, después de haber descartado la enfermedad celíaca, cuando el paciente sigue padeciendo molestias, se le examina con una prueba de anticuerpos de la IgE y una prueba de punción cutánea.
La alergia al trigo también puede parecerse a la SG/T por su cuadro clínico. Por eso, después de haber descartado la enfermedad celíaca, cuando el paciente sigue padeciendo molestias, se le examina con una prueba de anticuerpos de la IgE y una prueba de punción cutánea.
Indicios adicionales de la SG/T
Prueba de anticuerpos antigliadina (IgG)
Los anticuerpos antigliadina IgG (AGA) no son específicos únicamente de la SG/T, sino que también pueden detectarse en pacientes celíacos y en una pequeña parte de la población sana. Sin embargo, si el resultado histológico está dentro de lo normal y la prueba de anticuerpos AGA es positiva, la sospecha de una SG/T se corrobora.
Los anticuerpos antigliadina IgG (AGA) no son específicos únicamente de la SG/T, sino que también pueden detectarse en pacientes celíacos y en una pequeña parte de la población sana. Sin embargo, si el resultado histológico está dentro de lo normal y la prueba de anticuerpos AGA es positiva, la sospecha de una SG/T se corrobora.
Alimentación sin gluten
Mejoría de los síntomas
Si se ha descartado la enfermedad celíaca y la alergia al trigo, el paciente puede empezar a llevar una alimentación sin gluten. Si el paciente padece SG/T, los síntomas mejoran o desaparecen en un plazo que va de unos días a dos semanas. No obstante, debería continuarse con la alimentación sin gluten durante por lo menos seis semanas para establecer una conexión causal entre la alimentación sin gluten y las molestias. La mejoría de los síntomas debe evaluarse de acuerdo con un protocolo de diagnóstico elaborado en el International Expert Meeting 2014 para poder seguir un criterio estándar. Este protocolo exige que antes de empezar con la alimentación sin gluten el paciente identifique entre una y tres molestias principales y que las valore según un nivel de gravedad, basándose en una escala del uno al diez. Esta valoración debe llevarse a cabo dos semanas antes del inicio de la alimentación sin gluten y, a partir de entonces, cada semana. Una reacción satisfactoria a la alimentación sin gluten se muestra a través del siguiente criterio: X mejora en por lo menos un 30 % en comparación con el valor inicial, donde X equivale a cada una de las tres molestias principales. Como mínimo un síntoma debería mejorar, siempre y cuando el resto no empeoren. Esta mejoría debería alcanzar como mínimo el 50 % durante el periodo de evaluación.
Si se ha descartado la enfermedad celíaca y la alergia al trigo, el paciente puede empezar a llevar una alimentación sin gluten. Si el paciente padece SG/T, los síntomas mejoran o desaparecen en un plazo que va de unos días a dos semanas. No obstante, debería continuarse con la alimentación sin gluten durante por lo menos seis semanas para establecer una conexión causal entre la alimentación sin gluten y las molestias. La mejoría de los síntomas debe evaluarse de acuerdo con un protocolo de diagnóstico elaborado en el International Expert Meeting 2014 para poder seguir un criterio estándar. Este protocolo exige que antes de empezar con la alimentación sin gluten el paciente identifique entre una y tres molestias principales y que las valore según un nivel de gravedad, basándose en una escala del uno al diez. Esta valoración debe llevarse a cabo dos semanas antes del inicio de la alimentación sin gluten y, a partir de entonces, cada semana. Una reacción satisfactoria a la alimentación sin gluten se muestra a través del siguiente criterio: X mejora en por lo menos un 30 % en comparación con el valor inicial, donde X equivale a cada una de las tres molestias principales. Como mínimo un síntoma debería mejorar, siempre y cuando el resto no empeoren. Esta mejoría debería alcanzar como mínimo el 50 % durante el periodo de evaluación.
Reexposición al gluten
Confirmación del diagnóstico
Para confirmar el diagnóstico definitivo de la SG/T se lleva a cabo una nueva provocación similar a la realizada para una alergia alimentaria, es decir, el paciente vuelve a consumir gluten tras una fase estricta sin gluten que ha durado por lo menos cuatro semanas. Para realizar esta provocación, si es posible, debería comenzar una fase sin gluten de varios días, debería realizarse una provocación oral controlada mediante placebo en doble ciego (para estudios) o simple ciego (en el consultorio). Para esto, lo ideal es emplear barritas sin gluten (como placebo) y barritas con gluten que no puedan diferenciarse por su aspecto, textura y sabor. Tras una primera fase de una semana, se llevará a cabo una dieta sin gluten estricta durante una semana y una segunda fase de prueba de una semana. Una vez más el protocolo de diagnóstico estandarizado es la base para la valoración semanal de las molestias. Con una variación de como mínimo el 30 %, si aparecen entre uno y tres de los síntomas identificados por el paciente entre el suministro de gluten y el placebo, quiere decir que existe una SG/T.
Para confirmar el diagnóstico definitivo de la SG/T se lleva a cabo una nueva provocación similar a la realizada para una alergia alimentaria, es decir, el paciente vuelve a consumir gluten tras una fase estricta sin gluten que ha durado por lo menos cuatro semanas. Para realizar esta provocación, si es posible, debería comenzar una fase sin gluten de varios días, debería realizarse una provocación oral controlada mediante placebo en doble ciego (para estudios) o simple ciego (en el consultorio). Para esto, lo ideal es emplear barritas sin gluten (como placebo) y barritas con gluten que no puedan diferenciarse por su aspecto, textura y sabor. Tras una primera fase de una semana, se llevará a cabo una dieta sin gluten estricta durante una semana y una segunda fase de prueba de una semana. Una vez más el protocolo de diagnóstico estandarizado es la base para la valoración semanal de las molestias. Con una variación de como mínimo el 30 %, si aparecen entre uno y tres de los síntomas identificados por el paciente entre el suministro de gluten y el placebo, quiere decir que existe una SG/T.
Protocolo de diagnóstico para la sensibilidad al gluten/trigo
En la 3.ª edición del International Expert Meeting on Gluten Sensitivity en octubre de 2014 los científicos y médicos presentes desarrollaron el protocolo de diagnóstico descrito anteriormente bajo la supervisión de Carlo Catassi y Alessio Fasano. Este protocolo prevé un procedimiento estandarizado basado en dietas en dos fases, en el cual se emplea una versión modificada de la escala de valoración de síntomas gastrointestinales. Con esta escala los afectados valoran el efecto que tiene en ellos la introducción de una alimentación sin gluten y la reintroducción del gluten en sus molestias. No solo se valoran los síntomas gastrointestinales, sino también los extraintestinales, utilizando una escala de 1 a 10. A través de estos cuestionarios se logra una estandarización del diagnóstico.
Más información sobre este tema...
Download
2
Mostrar todo
Presentación
6
Mostrar todo
Estudios
3
Mostrar todo
Vídeos
2
Mostrar todo
Algoritmo trastornos relacionados con el gluten
Algoritmo diagnostico publicado por Ana Sapone en la revista BMC Medicine que permite la diferenciación de los trastornos funcionales relacionados con el gluten. Presenta las bases para llegar más fácilmente a un diagnóstico correcto distinguiendo la enfermedad celíaca de la sensibilidad al gluten o la alergia al trigo.

Resumen Expert Meeting GS 2012
Algoritmo trastornos relacionados con el gluten
Algoritmo diagnostico publicado por Ana Sapone en la revista BMC Medic...
How the diagnosis of non celiac gluten sensitivity should be confirmed: the Salerno experts’ criteria (2015)
Carlo Catassi
Department of Pediatrics
Università Politecnica delle Marche, Ancona
16th International Coeliac Disease Symposium 2015 a Praga
Pre-Conference Workshop on Gluten Sensitivity "The Evolving Planet of Gluten Related Disorders"
Department of Pediatrics
Università Politecnica delle Marche, Ancona
16th International Coeliac Disease Symposium 2015 a Praga
Pre-Conference Workshop on Gluten Sensitivity "The Evolving Planet of Gluten Related Disorders"
Biomarkers for Non-Celiac Gluten Sensitivity: A Tough, but Intriguing Challenge for Researchers (2015)
Umberto Volta
University of Bologna, Italy
16th International Coeliac Disease Symposium 2015 a Praga
Pre-Conference Workshop on Gluten Sensitivity "The Evolving Planet of Gluten Related Disorders"
University of Bologna, Italy
16th International Coeliac Disease Symposium 2015 a Praga
Pre-Conference Workshop on Gluten Sensitivity "The Evolving Planet of Gluten Related Disorders"
Diagnostic study of HLA-DQ2 typing for gluten sensitivity in IBS patients (2015)
Christian Barmeyer, Michael Schumann, Tim Meyer, Britta Siegmund, Severin Daum, Jörg-Dieter Schulzke, Reiner Ullrich
Medizinische Klinik für Gastroenterologie, Infektiologie und Rheumatologie
Charité - Universitätsmedizin Berlin
Campus Benjamin Franklin
16th International Coeliac Disease Symposium 2015 a Praga
Pre-Conference Workshop on Gluten Sensitivity "The Evolving Planet of Gluten Related Disorders"
Medizinische Klinik für Gastroenterologie, Infektiologie und Rheumatologie
Charité - Universitätsmedizin Berlin
Campus Benjamin Franklin
16th International Coeliac Disease Symposium 2015 a Praga
Pre-Conference Workshop on Gluten Sensitivity "The Evolving Planet of Gluten Related Disorders"
Gluten Sensitivity Biomarkers and Epidemiology, results from NHANES 2009–2010 (2013)
Peter H.R. Green
Celiac Disease Center
Columbia University
New York, USA
15. International Celiac Disease Symposium del 22 y el 25 de septiembre de 2013, Chicago
Celiac Disease Center
Columbia University
New York, USA
15. International Celiac Disease Symposium del 22 y el 25 de septiembre de 2013, Chicago
Gluten Sensitivity: Biomarkers and Epidemiology. The Ongoing Field Experience (2013)
Umberto Volta
Coordinator of Italian Celiac Association Board
Department of Medical and Surgical Sciences
University of Bologna, Italy
15. International Celiac Disease Symposium del 22 y el 25 de septiembre de 2013, Chicago
Coordinator of Italian Celiac Association Board
Department of Medical and Surgical Sciences
University of Bologna, Italy
15. International Celiac Disease Symposium del 22 y el 25 de septiembre de 2013, Chicago

Management of Gluten Sensitivity: Nutritional Management (2013)
Pam Cureton, RD, LD
Dietitian
Center for Celiac Research & Treatment
Boston MA, USA
15. International Celiac Disease Symposium del 22 y el 25 de septiembre de 2013, Chicago
Dietitian
Center for Celiac Research & Treatment
Boston MA, USA
15. International Celiac Disease Symposium del 22 y el 25 de septiembre de 2013, Chicago
How the diagnosis of non celiac gluten sensitivity should be confirmed: the Salerno experts’ criteria (2015)
Carlo Catassi
Department of Pediatrics
Università Politecnica delle ...
Biomarkers for Non-Celiac Gluten Sensitivity: A Tough, but Intriguing Challenge for Researchers (2015)
Umberto Volta
University of Bologna, Italy
16th International Coel...
Diagnostic study of HLA-DQ2 typing for gluten sensitivity in IBS patients (2015)
Christian Barmeyer, Michael Schumann, Tim Meyer, Britta Siegmund, Seve...
Gluten Sensitivity Biomarkers and Epidemiology, results from NHANES 2009–2010 (2013)
Peter H.R. Green
Celiac Disease Center
Columbia University
New York...
Gluten Sensitivity: Biomarkers and Epidemiology. The Ongoing Field Experience (2013)
Umberto Volta
Coordinator of Italian Celiac Association Board
Depart...
Management of Gluten Sensitivity: Nutritional Management (2013)
Pam Cureton, RD, LD
Dietitian
Center for Celiac Research & Treatment...

Diagnosis of Non-Celiac Gluten Sensitivity (NCGS): The Salerno Experts’ Criteria
Abstract
Non-Celiac Gluten Sensitivity (NCGS) is a syndrome characterized by intestinal and extra-intestinal symptoms related to the ingestion of gluten-containing food, in subjects that are not affected by either celiac disease or wheat allergy. Given the lack of a NCGS biomarker, there is the need for standardizing the procedure leading to the diagnosis confirmation. In this paper we report experts’ recommendations on how the diagnostic protocol should be performed for the confirmation of NCGS. A full diagnostic procedure should assess the clinical response to the gluten-free diet (GFD) and measure the effect of a gluten challenge after a period of treatment with the GFD. The clinical evaluation is performed using a self-administered instrument incorporating a modified version of the Gastrointestinal Symptom Rating Scale. The patient identifies one to three main symptoms that are quantitatively assessed using a Numerical Rating Scale with a score ranging from 1 to 10. The double-blind placebo-controlled gluten challenge (8 g/day) includes a one-week challenge followed by a one-week washout of strict GFD and by the crossover to the second one-week challenge. The vehicle should contain cooked, homogeneously distributed gluten. At least a variation of 30% of one to three main symptoms between the gluten and the placebo challenge should be detected to discriminate a positive from a negative result. The guidelines provided in this paper will help the clinician to reach a firm and positive diagnosis of NCGS and facilitate the comparisons of different studies, if adopted internationally.
Resource: Nutrients 2015, 7(6), 4966-4977; doi:10.3390/nu7064966
Carlo Catassi, Luca Elli, Bruno Bonaz, Gerd Bouma, Antonio Carroccio, Gemma Castillejo, Christophe Cellier, Fernanda Cristofori, Laura de Magistris, Jernej Dolinsek, Walburga Dieterich, Ruggiero Francavilla, Marios Hadjivassiliou, Wolfgang Holtmeier, Ute Körner, Dan A. Leffler,Knut E. A. Lundin, Giuseppe Mazzarella, Chris J. Mulder, Nicoletta Pellegrini, Kamran Rostami, David Sanders, Gry Irene Skodje, Detlef Schuppan, Reiner Ullrich, Umberto Volta, Marianne Williams, Victor F. Zevallos, Yurdagül Zopf and Alessio Fasano
Non-Celiac Gluten Sensitivity (NCGS) is a syndrome characterized by intestinal and extra-intestinal symptoms related to the ingestion of gluten-containing food, in subjects that are not affected by either celiac disease or wheat allergy. Given the lack of a NCGS biomarker, there is the need for standardizing the procedure leading to the diagnosis confirmation. In this paper we report experts’ recommendations on how the diagnostic protocol should be performed for the confirmation of NCGS. A full diagnostic procedure should assess the clinical response to the gluten-free diet (GFD) and measure the effect of a gluten challenge after a period of treatment with the GFD. The clinical evaluation is performed using a self-administered instrument incorporating a modified version of the Gastrointestinal Symptom Rating Scale. The patient identifies one to three main symptoms that are quantitatively assessed using a Numerical Rating Scale with a score ranging from 1 to 10. The double-blind placebo-controlled gluten challenge (8 g/day) includes a one-week challenge followed by a one-week washout of strict GFD and by the crossover to the second one-week challenge. The vehicle should contain cooked, homogeneously distributed gluten. At least a variation of 30% of one to three main symptoms between the gluten and the placebo challenge should be detected to discriminate a positive from a negative result. The guidelines provided in this paper will help the clinician to reach a firm and positive diagnosis of NCGS and facilitate the comparisons of different studies, if adopted internationally.
Resource: Nutrients 2015, 7(6), 4966-4977; doi:10.3390/nu7064966
Carlo Catassi, Luca Elli, Bruno Bonaz, Gerd Bouma, Antonio Carroccio, Gemma Castillejo, Christophe Cellier, Fernanda Cristofori, Laura de Magistris, Jernej Dolinsek, Walburga Dieterich, Ruggiero Francavilla, Marios Hadjivassiliou, Wolfgang Holtmeier, Ute Körner, Dan A. Leffler,Knut E. A. Lundin, Giuseppe Mazzarella, Chris J. Mulder, Nicoletta Pellegrini, Kamran Rostami, David Sanders, Gry Irene Skodje, Detlef Schuppan, Reiner Ullrich, Umberto Volta, Marianne Williams, Victor F. Zevallos, Yurdagül Zopf and Alessio Fasano

Celiac Disease or Non-Celiac Gluten Sensitivity? An Approach to Clinical Differential Diagnosis
Abstract
OBJECTIVES: Differentiating between celiac disease (CD) and non-celiac gluten sensitivity (NCGS) is important for appropriate management but is often challenging.
METHODS: We retrospectively reviewed records from 238 patients who presented for the evaluation of symptoms responsive to gluten restriction without prior diagnosis or exclusion of CD. Demographics, presenting symptoms, serologic, genetic, and histologic data, nutrient deficiencies, personal history of autoimmune diseases, and family history of CD were recorded. NCGS was defined as symptoms responsive to a gluten-free diet (GFD) in the setting of negative celiac serology and duodenal biopsies while on a gluten-containing diet or negative human leukocyte antigen (HLA) DQ2/DQ8 testing.
RESULTS: Of the 238 study subjects, 101 had CD, 125 had NCGS, 9 had non-celiac enteropathy, and 3 had indeterminate diagnosis. CD subjects presented with symptoms of malabsorption 67.3% of the time compared with 24.8% of the NCGS subjects (P<0.0001). In addition, CD subjects were significantly more likely to have a family history of CD (P=0.004), personal history of autoimmune diseases (P=0.002), or nutrient deficiencies (P<0.0001). The positive likelihood ratio for diagnosis of CD of a >2× upper limit of normal IgA trans-glutaminase antibody (tTG) or IgA/IgG deaminated gliadan peptide antibody (DGP) with clinical response to GFD was 130 (confidence interval (CI): 18.5–918.3). The positive likelihood ratio of the combination of gluten-responsive symptoms and negative IgA tTG or IgA/IgG DGP on a regular diet for NCGS was 9.6 (CI: 5.5–16.9). When individuals with negative IgA tTG or IgA/IgG DGP also lacked symptoms of malabsorption (weight loss, diarrhea, and nutrient deficiencies) and CD risk factors (personal history of autoimmune diseases and family history of CD), the positive likelihood ratio for NCGS increased to 80.9.
CONCLUSIONS: On the basis of our findings, we have developed a diagnostic algorithm to differentiate CD from NCGS. Subjects with negative celiac serologies (IgA tTG or IgA/IgG DGP) on a regular diet are unlikely to have CD. Those with negative serology who also lack clinical evidence of malabsorption and CD risk factors are highly likely to have NCGS and may not require further testing. Those with equivocal serology should undergo HLA typing to determine the need for biopsy.
Resource: The American Journal of Gastroenterology 109, 741-746 (May 2014)
Toufic A Kabbani, Rohini R Vanga, Daniel A Leffler, Javier Villafuerte-Galvez, Kumar Pallav, Joshua Hansen, Rupa Mukherjee, Melinda Dennis and Ciaran P Kelly
OBJECTIVES: Differentiating between celiac disease (CD) and non-celiac gluten sensitivity (NCGS) is important for appropriate management but is often challenging.
METHODS: We retrospectively reviewed records from 238 patients who presented for the evaluation of symptoms responsive to gluten restriction without prior diagnosis or exclusion of CD. Demographics, presenting symptoms, serologic, genetic, and histologic data, nutrient deficiencies, personal history of autoimmune diseases, and family history of CD were recorded. NCGS was defined as symptoms responsive to a gluten-free diet (GFD) in the setting of negative celiac serology and duodenal biopsies while on a gluten-containing diet or negative human leukocyte antigen (HLA) DQ2/DQ8 testing.
RESULTS: Of the 238 study subjects, 101 had CD, 125 had NCGS, 9 had non-celiac enteropathy, and 3 had indeterminate diagnosis. CD subjects presented with symptoms of malabsorption 67.3% of the time compared with 24.8% of the NCGS subjects (P<0.0001). In addition, CD subjects were significantly more likely to have a family history of CD (P=0.004), personal history of autoimmune diseases (P=0.002), or nutrient deficiencies (P<0.0001). The positive likelihood ratio for diagnosis of CD of a >2× upper limit of normal IgA trans-glutaminase antibody (tTG) or IgA/IgG deaminated gliadan peptide antibody (DGP) with clinical response to GFD was 130 (confidence interval (CI): 18.5–918.3). The positive likelihood ratio of the combination of gluten-responsive symptoms and negative IgA tTG or IgA/IgG DGP on a regular diet for NCGS was 9.6 (CI: 5.5–16.9). When individuals with negative IgA tTG or IgA/IgG DGP also lacked symptoms of malabsorption (weight loss, diarrhea, and nutrient deficiencies) and CD risk factors (personal history of autoimmune diseases and family history of CD), the positive likelihood ratio for NCGS increased to 80.9.
CONCLUSIONS: On the basis of our findings, we have developed a diagnostic algorithm to differentiate CD from NCGS. Subjects with negative celiac serologies (IgA tTG or IgA/IgG DGP) on a regular diet are unlikely to have CD. Those with negative serology who also lack clinical evidence of malabsorption and CD risk factors are highly likely to have NCGS and may not require further testing. Those with equivocal serology should undergo HLA typing to determine the need for biopsy.
Resource: The American Journal of Gastroenterology 109, 741-746 (May 2014)
Toufic A Kabbani, Rohini R Vanga, Daniel A Leffler, Javier Villafuerte-Galvez, Kumar Pallav, Joshua Hansen, Rupa Mukherjee, Melinda Dennis and Ciaran P Kelly
Characterization of Adults With a Self-Diagnosis of Nonceliac Gluten Sensitivity
Abstract
Background: Nonceliac gluten sensitivity (NCGS), occurring in patients without celiac disease yet whose gastrointestinal symptoms improve on a gluten-free diet (GFD), is largely a self-reported diagnosis and would appear to be very common. The aims of this study were to characterize patients who believe they have NCGS.
Materials and Methods: Advertising was directed toward adults who believed they had NCGS and were willing to participate in a clinical trial. Respondents were asked to complete a questionnaire about symptoms, diet, and celiac investigation.
Results: Of 248 respondents, 147 completed the survey. Mean age was 43.5 years, and 130 were women. Seventy-two percent did not meet the description of NCGS due to inadequate exclusion of celiac disease (62%), uncontrolled symptoms despite gluten restriction (24%), and not following a GFD (27%), alone or in combination. The GFD was self-initiated in 44% of respondents; in other respondents it was prescribed by alternative health professionals (21%), dietitians (19%), and general practitioners (16%). No celiac investigations had been performed in 15% of respondents. Of 75 respondents who had duodenal biopsies, 29% had no or inadequate gluten intake at the time of endoscopy. Inadequate celiac investigation was common if the GFD was initiated by self (69%), alternative health professionals (70%), general practitioners (46%), or dietitians (43%). In 40 respondents who fulfilled the criteria for NCGS, their knowledge of and adherence to the GFD were excellent, and 65% identified other food intolerances.
Conclusions: Just over 1 in 4 respondents self-reporting as NCGS fulfill criteria for its diagnosis. Initiation of a GFD without adequate exclusion of celiac disease is common. In 1 of 4 respondents, symptoms are poorly controlled despite gluten avoidance.
Resource: Nutr Clin Pract April 16, 2014
Jessica R. Biesiekierski, PhD, RN, Evan D. Newnham , MD, FRACP, Susan J. Shepherd, PhD, APD, Jane G. Muir, PhD, APD, Peter R. Gibson, MD, FRACP
Background: Nonceliac gluten sensitivity (NCGS), occurring in patients without celiac disease yet whose gastrointestinal symptoms improve on a gluten-free diet (GFD), is largely a self-reported diagnosis and would appear to be very common. The aims of this study were to characterize patients who believe they have NCGS.
Materials and Methods: Advertising was directed toward adults who believed they had NCGS and were willing to participate in a clinical trial. Respondents were asked to complete a questionnaire about symptoms, diet, and celiac investigation.
Results: Of 248 respondents, 147 completed the survey. Mean age was 43.5 years, and 130 were women. Seventy-two percent did not meet the description of NCGS due to inadequate exclusion of celiac disease (62%), uncontrolled symptoms despite gluten restriction (24%), and not following a GFD (27%), alone or in combination. The GFD was self-initiated in 44% of respondents; in other respondents it was prescribed by alternative health professionals (21%), dietitians (19%), and general practitioners (16%). No celiac investigations had been performed in 15% of respondents. Of 75 respondents who had duodenal biopsies, 29% had no or inadequate gluten intake at the time of endoscopy. Inadequate celiac investigation was common if the GFD was initiated by self (69%), alternative health professionals (70%), general practitioners (46%), or dietitians (43%). In 40 respondents who fulfilled the criteria for NCGS, their knowledge of and adherence to the GFD were excellent, and 65% identified other food intolerances.
Conclusions: Just over 1 in 4 respondents self-reporting as NCGS fulfill criteria for its diagnosis. Initiation of a GFD without adequate exclusion of celiac disease is common. In 1 of 4 respondents, symptoms are poorly controlled despite gluten avoidance.
Resource: Nutr Clin Pract April 16, 2014
Jessica R. Biesiekierski, PhD, RN, Evan D. Newnham , MD, FRACP, Susan J. Shepherd, PhD, APD, Jane G. Muir, PhD, APD, Peter R. Gibson, MD, FRACP
Diagnosis of Non-Celiac Gluten Sensitivity (NCGS): The Salerno Experts’ Criteria
Abstract
Non-Celiac Gluten Sensitivity (NCGS) is a syndrome character...
Celiac Disease or Non-Celiac Gluten Sensitivity? An Approach to Clinical Differential Diagnosis
Abstract
OBJECTIVES: Differentiating between celiac disease (CD) an...
Characterization of Adults With a Self-Diagnosis of Nonceliac Gluten Sensitivity
Abstract
Background: Nonceliac gluten sensitivity (NCGS), occurring...
NCGS: are we moving from a diagnosis of exclusion to a positive diagnosis?
Professor Carlo Catassi
Gastroenterologist Pediatrician
Department of Pediatrics
Università Politecnica delle Marche
60123 Ancona, Italy
At the Expert Meeting 2014 in Salerno, Italy.
Gastroenterologist Pediatrician
Department of Pediatrics
Università Politecnica delle Marche
60123 Ancona, Italy
At the Expert Meeting 2014 in Salerno, Italy.
Are we moving from a diagnosis of exclusion to a positive diagnosis?
Reiner Ullrich, MD
Universitätsmedizin Berlin
Campus Benjamin Franklin,
Medizinische Klinik für Gastroenterologie
12203 Berlin, Germany
At the Expert Meeting 2014 in Salerno, Italy
Universitätsmedizin Berlin
Campus Benjamin Franklin,
Medizinische Klinik für Gastroenterologie
12203 Berlin, Germany
At the Expert Meeting 2014 in Salerno, Italy
NCGS: are we moving from a diagnosis of exclusion to a positive diagnosis?
Professor Carlo Catassi
Gastroenterologist Pediatrician
Department o...
Are we moving from a diagnosis of exclusion to a positive diagnosis?
Reiner Ullrich, MD
Universitätsmedizin Berlin
Campus Benjamin Frankl...
www.drschaer-institute.com