The Global Map of Coeliac Disease

This article focuses on the worldwide epidemiology of coeliac disease. The information it contains is not only relevant for statistical purposes but also serves to formulate hypotheses on the factors which contribute to the development of this disease that is so widespread in modern society.
The development of simple but reliable diagnostic tests, making it possible to analyse the frequency of coeliac disease in different population groups and geographical regions, has hugely assisted epidemiological research in this field. These methods – including the detection of anti-transglutaminase antibodies and anti-endomysial antibodies as well as the HLA test for genetic predisposition – require just a few drops of blood. This international research has resulted in an interesting global map of coeliac disease which we will now consider in a little more detail.
Coeliac disease used to be considered a rare disease limited almost exclusively to those of European origin and in paediatric patients. However, the first serological tests, launched in the 1980s, have revealed a very different reality. Coeliac disease is one of the most frequent of all lifelong diseases, affecting children and adults in equal measure and has been shown to be more common in women (ratio men / women = 1:1.5-2). In Italy, and generally in Europe, where most research into coeliac disease has been carried out, around 1 % of the population is affected, although there are major differences between the different European countries: in Germany only 0.2 % of the population suffer from coeliac disease, whilst in Finland this figure is over 2 %. As the genetic differences between these populations are very small, it can be assumed that these fluctuations in frequency are the result of still relatively unknown environmental factors such as child nutrition, intestinal infections and the typology of intestinal flora (known as “microbiome”). Other countries with populations of primarily European descent – such as the United States, Australia and Argentina – have also shown an average frequency of 1 %.
Coeliac disease used to be considered a rare disease limited almost exclusively to those of European origin and in paediatric patients. However, the first serological tests, launched in the 1980s, have revealed a very different reality. Coeliac disease is one of the most frequent of all lifelong diseases, affecting children and adults in equal measure and has been shown to be more common in women (ratio men / women = 1:1.5-2). In Italy, and generally in Europe, where most research into coeliac disease has been carried out, around 1 % of the population is affected, although there are major differences between the different European countries: in Germany only 0.2 % of the population suffer from coeliac disease, whilst in Finland this figure is over 2 %. As the genetic differences between these populations are very small, it can be assumed that these fluctuations in frequency are the result of still relatively unknown environmental factors such as child nutrition, intestinal infections and the typology of intestinal flora (known as “microbiome”). Other countries with populations of primarily European descent – such as the United States, Australia and Argentina – have also shown an average frequency of 1 %.
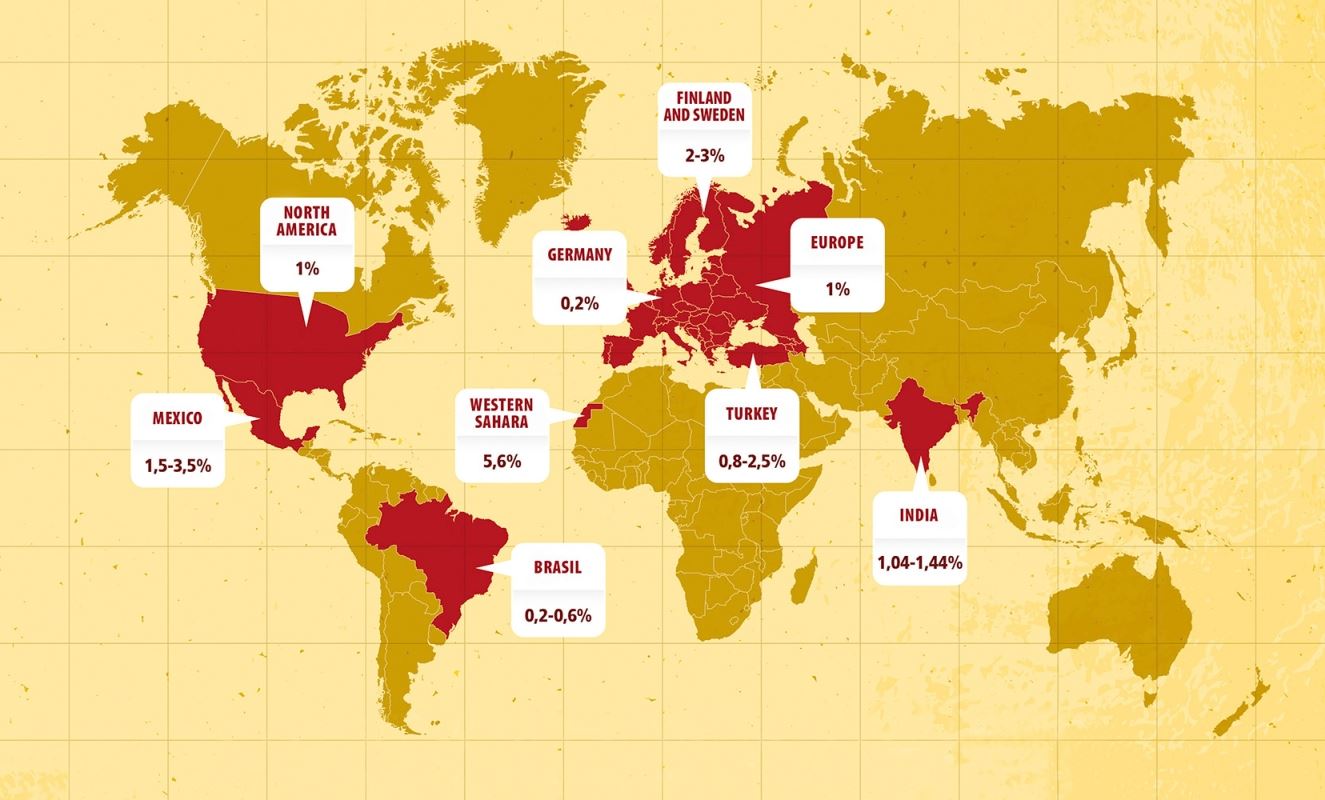
Map showing the epidemiology & geography of modern coeliac disease
Another worrying fact revealed by epidemiological research is that frequency of coeliac disease is still on the rise in the West. In the United States, for example, the frequency has increased over the last 40 years from 2 cases per thousand to 10 cases per thousand (1 %). This alarming fact also indicates that environmental factors, play a decisive role.
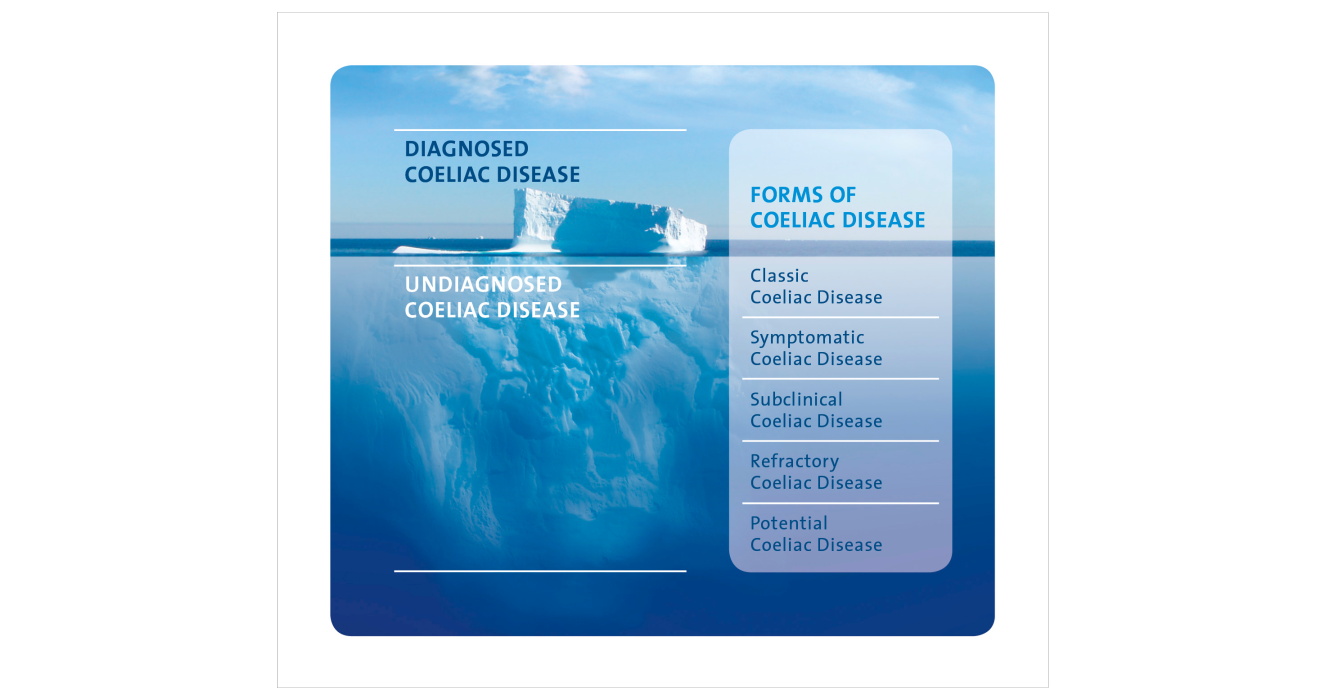
At the same time as this epidemiological research was being undertaken, the concept of the “coeliac iceberg” developed. This represents the current epidemiological situation that, despite an ongoing rise in diagnosed cases, the number of coeliac sufferers still to be diagnosed is still a long way below previous estimates of the total prevalence. Approximately 70-80 % of all cases remain undiagnosed (representing the section of the iceberg below the water’s surface), which may be due to sufferers experiencing either ambiguous symptoms or no symptoms at all. In such situations there is a risk that patients may later suffer from complications associated with coeliac disease as a result of not receiving dietary treatment for the condition.
In developing countries the epidemiological reality is far more concerning than in the Western world. First and foremost, the myth that coeliac disease primarily affects Europe-ans has been disproved: research indicates that the frequency of the disease in North Africa, the Middle East and India is the same (around 1 %) as in Europe. Indeed, in one group of African people – the Sahrawi from the Western Sahara – coeliac disease was shown to have an endemic presence of 6-7 % among children. The reasons for such a high frequency are unknown; however, it is believed that this specific situation may have been caused by a sudden change in the Sahrawi’s eating habits that saw them switch from a diet of mainly camel milk and camel meat to more Europe-an eating habits, including a drastic increase in their consumption of cereal products, as a result of Spanish colonisation. In developing countries, non-diagnosed cases of coeliac disease can cause severe forms of protein-energy malnutrition, which in turn increases the risk of other diseases and infant mortality. The lack of awareness among doctors about coeliac disease and the limited availability of diagnostic tests mean that the diagnosed cases of the disease represent only a fraction of the total number of people affected. In India, for ex-ample, it is estimated that, as well as the few thousand diagnosed cases, there are a further 5-10 million who have coeliac disease (a “coe-liac iceberg” that lies almost entirely below the water’s surface).
At the same time as this epidemiological research was being undertaken, the concept of the “coeliac iceberg” developed. This represents the current epidemiological situation that, despite an ongoing rise in diagnosed cases, the number of coeliac sufferers still to be diagnosed is still a long way below previous estimates of the total prevalence. Approximately 70-80 % of all cases remain undiagnosed (representing the section of the iceberg below the water’s surface), which may be due to sufferers experiencing either ambiguous symptoms or no symptoms at all. In such situations there is a risk that patients may later suffer from complications associated with coeliac disease as a result of not receiving dietary treatment for the condition.
In developing countries the epidemiological reality is far more concerning than in the Western world. First and foremost, the myth that coeliac disease primarily affects Europe-ans has been disproved: research indicates that the frequency of the disease in North Africa, the Middle East and India is the same (around 1 %) as in Europe. Indeed, in one group of African people – the Sahrawi from the Western Sahara – coeliac disease was shown to have an endemic presence of 6-7 % among children. The reasons for such a high frequency are unknown; however, it is believed that this specific situation may have been caused by a sudden change in the Sahrawi’s eating habits that saw them switch from a diet of mainly camel milk and camel meat to more Europe-an eating habits, including a drastic increase in their consumption of cereal products, as a result of Spanish colonisation. In developing countries, non-diagnosed cases of coeliac disease can cause severe forms of protein-energy malnutrition, which in turn increases the risk of other diseases and infant mortality. The lack of awareness among doctors about coeliac disease and the limited availability of diagnostic tests mean that the diagnosed cases of the disease represent only a fraction of the total number of people affected. In India, for ex-ample, it is estimated that, as well as the few thousand diagnosed cases, there are a further 5-10 million who have coeliac disease (a “coe-liac iceberg” that lies almost entirely below the water’s surface).
Considering this situation, it seems right to ask which strategy represents the most effec-tive way of bringing such undiagnosed cases “to the surface”. So far, the strategy most commonly recommended has been to use the diagnostic tests on all persons who are “at risk”, for example relatives of people with coeliac disease as well as individuals with autoimmune diseases or with symptoms that may indicate the presence of coeliac disease (stunted growth, persistent intestinal problems, anaemia, etc.). This low-cost strategy, known as “case-finding”, can be justified from both an ethical and a financial point of view, but it is not particularly effective and diagnoses no more than 30 % of cases. Therefore, “universal” screening is gaining ground. In this case, blood tests could be carried out on all children when they reach the age of compulsory education (5 years) in order to determine the presence of coeliac antibodies. The effectiveness of this strategy may be linked to the fact that the child’s genetic predisposition could already have been assessed at birth (the HLA test, like other screening methods used on new-borns, requires just a drop of blood), so antibody tests are carried out only on those children who tested positive for a genetic predisposition to the disease at birth.
In conclusion, it can be confirmed that the global map of coeliac disease is far more densely “populated” than previously assumed. Health authorities both in the Western world and in developing countries must pay serious attention to this situation. Epidemiological research into coeliac disease contributes to identifying the environmental factors that may be responsible for fluctuations in frequency. In practice, it is necessary to raise awareness of this “chameeleon-like” disease as well as to develop possible mass-screening strategies in order to bring those many undiagnosed cases to point of diagnosis.
In conclusion, it can be confirmed that the global map of coeliac disease is far more densely “populated” than previously assumed. Health authorities both in the Western world and in developing countries must pay serious attention to this situation. Epidemiological research into coeliac disease contributes to identifying the environmental factors that may be responsible for fluctuations in frequency. In practice, it is necessary to raise awareness of this “chameeleon-like” disease as well as to develop possible mass-screening strategies in order to bring those many undiagnosed cases to point of diagnosis.
Author
PROFESSOR CARLO CATASSI
- Professor for pediatrician at the Marche Poltechnic University (Italy)
- President of the Italian Society for Pediatric Gastroenterology, Hepatology and Nutrition, years 2013-2016
- Coordinator of the Dr. Schär Advisory Board
References
- Catassi C, Gatti S, Fasano A “The New Epidemiology of Coeliac Disease” Journal of Pediatric Gastroenterology & Nutrition, July 2014 Volume 59
www.drschaer-institute.com